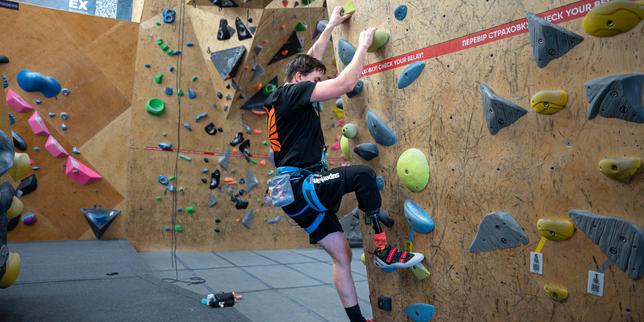
The chalk dust hangs in the air like heavy winter mist. It clings to the sweat on Oleksandr’s forehead, settling into the deep lines etched there by things he prefers not to name. He reaches upward. His right hand grips a brightly colored resin hold, shaped like a jagged rock. He pulls. His left leg, a masterpiece of carbon fiber, titanium, and shock-absorbing plastics, presses against the plywood wall. The prosthetic squeaks against the grain.
Gravity is an absolute dictator. It does not care about geopolitics. It does not care about heroism. It only demands weight, and on a vertical climbing wall in Kyiv, weight is the only currency that matters.
For months, Oleksandr’s world was horizontal. It was a world of sterile hospital ceilings, the soft squeak of nurses’ thick-soled shoes, and the agonizingly slow rhythm of a healing stump. When an anti-personnel mine took his leg near Bakhmut, it also took his relationship with space. To be bedridden is to be defeated by the earth.
But here, three meters above the safety mats, the horizontal world disappears. There is only the next hold. There is only the immediate, desperate requirement of balance.
The Phantom Limb and the Concrete Wall
When a soldier loses a limb to modern artillery, the trauma extends far beyond the surgical amputation. The brain retains a ghost map of what used to be there. For many Ukrainian veterans, this manifests as a cruel irony: a foot that no longer exists can still feel like it is burning, or clenching, or trapped under frozen mud.
Neurologists call this phantom limb pain. Veterans call it hell.
Medical facilities can prescribe gabapentin, mirror therapy, and heavy analgesics. These tools have their place. Yet, traditional rehabilitation often recreates the atmosphere of helplessness. You sit on a examination table. A physical therapist moves your residual limb. You are a patient. You are broken.
Climbing shatters that dynamic.
Consider the mechanics of ascending a wall. When a climber with an amputation engages with a route, the brain faces a massive, complex spatial puzzle. It must calculate how to balance without a calf muscle to flex or an ankle to rotate. The sensory overload is immense. The forearm muscles scream. The core tightens. The nervous system is so flooded with immediate, real-time data that the ghost signals of the phantom limb are suddenly drowned out.
The brain gets hijacked by survival. In that beautiful, focused panic, the phantom pain vanishes.
It is not a cure. It is a truce. But for someone who has not slept a full night in a year because their missing toes feel like they are being crushed by pliers, a two-hour truce is a miracle.
Reclaiming the Chemical Surge
There is a specific cocktail of chemicals that the human body secretes when it believes death is a distinct possibility. Adrenaline spikes the heart rate. Cortisol sharpens the vision. Endorphins numb the flesh.
Soldiers become intimately familiar with this rush. They live on it for months, sometimes years, in the trenches. Then, abruptly, they are discharged. They return to a quiet apartment in a city that is trying to pretend things are normal. The silence is deafening. The lack of danger feels less like peace and more like a sensory deprivation chamber.
This is where the psychological trap springs shut. The civilian world feels flat, meaningless, and gray.
"The adrenaline makes me feel whole again," Oleksandr says, his voice dropping to a rough whisper. He is not talking about the destructive thrill of combat. He is talking about the clean, controlled terror of the high wall.
When you are climbing, your body experiences the exact same physiological cascade as it does under fire. Your heart hammers against your ribs. Your breath becomes shallow. Your pupils dilate. But the context is entirely inverted. On the wall, the adrenaline is not a harbinger of shrapnel and death. It is the fuel used to conquer a physical obstacle.
It allows a veteran to experience intensity without trauma. It re-contextualizes the chemical fire inside their nervous system, transforming it from a symptom of post-traumatic stress into a tool for athletic achievement. They are no longer victims of an explosion; they are athletes negotiating with gravity.
The Weight of the Carbon Fiber
Adapting to a prosthetic leg on flat ground is a grueling chore. The gait is mechanical. Every step requires conscious thought. You must lift the hip slightly higher to clear the toe. You must trust a hinge made in a factory to support your entire existence.
On a vertical plane, that relationship becomes deeply complicated.
Prosthetic feet designed for walking are flat. They are meant to roll from heel to toe. Climbing holds, however, are often no wider than a coin. A climber must learn to use the edge of a carbon-fiber blade, wedging it into tiny crevices, relying entirely on friction and the strength of their remaining thigh muscles.
Let us look at the physics. A standard human foot has dozens of bones, tendons, and nerve endings that constantly send micro-signals to the brain, adjusting balance by millimeters. A prosthetic offers zero sensory feedback. When Oleksandr places his artificial foot on a hold, he cannot feel if it is secure. He has to watch it. He has to trust his eyes because his nerves are blind.
This creates a hyper-focus that is exhausting. Every movement is a calculated risk. If the foot slips, the fall is immediate.
Yet, watch a group of these men and women in a gym in Kyiv or Lviv, and the atmosphere is devoid of pity. There is a sharp, dark humor that only those who have looked into the abyss can manage. When someone’s prosthetic falls off mid-climb and dangles from the safety harness like a bizarre pendulum, the gym does not fall silent. It erupts into laughter.
That laughter is a shield. It is proof that the injury has lost its power to terrify.
Beyond the Clinical Horizon
The traditional model of veteran care is often insular. It takes place in white rooms, behind closed doors, surrounded by other wounded individuals. It can feel like a ghetto of grief.
Climbing gyms are fundamentally public spaces. They are noisy, vibrant hubs filled with teenagers, tech workers, and professional athletes. When a veteran ties into a rope next to a civilian who is warming up for a casual evening climb, something subtle changes in the room's gravity.
There is no need for a tearful conversation about what happened in the east. The shared language is written on the wall. Both individuals are looking at the same route, struggling with the same cruel slopers and dynamic moves. The veteran is not an object of charity; they are a peer on the rock.
This integration is the true objective of rehabilitation. It moves the individual from a state of being "the wounded soldier" to simply being "the climber in the red shirt." The disability becomes a secondary characteristic, a logistical detail to be managed rather than a defining identity.
The sun begins to dip below the horizon, casting long, sharp shadows across the plywood walls of the gym. Oleksandr lowers back to the mat. His forearms are swollen with blood, a deep, satisfying ache that signifies effort rather than injury. He unclips his harness with practiced efficiency.
He sits on a wooden bench and unstraps the carbon-fiber leg, letting the skin of his residual limb breathe. The silicone liner is soaked with sweat.
He looks up at the top of the route he just completed. A small piece of blue tape marks the final hold, fifteen meters above the ground. His hands are white with chalk, skin raw, fingers trembling slightly from the exertion.
For the first time all day, his mind is completely quiet. The ghost in his leg is silent. The war is still out there, heavy and unresolved, but for the next few hours, the only direction that matters is up.



